Scoliosis and Spine

Scoliosis & Spine Care at Scottish Rite for Children
The Spine Care Program at Scottish Rite offers world-class care for children with spinal conditions. Our experts practice team medicine, which means our patients have access to a group of in-house specialists including surgeons, psychologists, orthotists, physical therapists, child life specialists and more. This team approach allows us to provide personalized care for every patient, making sure they receive the support they need to grow, move and get back to doing what they love.
About Scoliosis
Scoliosis is when the spine curves or twists to the side, forming a C or S shape. It usually gets worse over time, making it a progressive condition. Around 2% to 3% of kids and teens are diagnosed with scoliosis.
The condition can affect different parts of the spine:
- Lumbar scoliosis affects the lower back.
- Thoracic scoliosis occurs in the middle of the spine.
- Thoracolumbar scoliosis impacts both the lower and middle sections.
Scoliosis is more common in girls, but it can affect any child. Most of the time, there’s no clear reason why it happens. However, a family history of scoliosis increases a child’s risk of developing the condition.
Here are a few important things to know:
- In congenital scoliosis, the cause is known. Some kids are born with a misshaped vertebra, or the curve may be linked to a neurological condition (neuromuscular scoliosis).
- Things like slouching, bad posture, sleeping positions, not getting enough calcium, or carrying heavy backpacks don’t cause scoliosis. It’s not because of anything a child did, and there’s no way to prevent it.
- Researchers at Scottish Rite are working to find out what causes scoliosis, why some curves worsen, how to slow it down and ways to improve treatment.
Our collaborative approach to treating spinal conditions is unique. For example, if a patient needs a scoliosis brace, their custom brace will be made by our on-site orthotics team, and an orthotists will be present at each of the patient’s clinic visits to assess the brace and make any adjustments.
Child Life specialists and physical therapists are also part of our care team, helping children and families feel comfortable and supported throughout their journey.
There are several types of scoliosis:
- Adolescent idiopathic scoliosis is the most common type of scoliosis in children and teens. It develops between the ages of 10 and 18. Idiopathic means there is no known cause, and it occurs in children who do not have any other medical problems.
- Congenital scoliosis is present from birth and involves abnormal development of the small bones in the spine, called vertebrae, before a child is born.
- Early-onset scoliosis (EOS) is a side-to-side (lateral) curve of the spine diagnosed in children 8 and under.
- Neuromuscular and syndromic scoliosis happens in children with another medical condition that affects the muscles, nerves or spine, such as cerebral palsy, muscular dystrophy, spinal muscular atrophy or spina bifida.
Scoliosis is more common in girls, but any child can develop the condition. In most cases, there is no known cause. However, a family history of scoliosis increases a child’s risk of developing the condition.
In congenital scoliosis, the cause is known. A child may be born with a misshapen vertebra, one of the building blocks of the spine. A curve may also develop from an underlying neurological disorder (neuromuscular scoliosis).
Slouching, bad posture, sleeping position, lack of calcium or carrying heavy books, backpacks or purses does not cause scoliosis. It’s not the result of doing anything “wrong,” and there’s no way to prevent it.
Groundbreaking research at Scottish Rite for Children is working to determine the cause of scoliosis, better understand factors that lead to curve progression, explore ways to prevent curve progression and improve treatments.
Scoliosis is usually diagnosed during a routine physical exam with a pediatrician or a school screening. The most common test for scoliosis is the Adam’s forward bend test. During this exam, the child bends forward while an examiner looks for signs of scoliosis in the back.
Scoliosis can range from mild to severe. Signs include:
- One hip that appears higher than the other
- One shoulder blade that is more prominent than the other
- Uneven shoulders
- An asymmetrical rib cage in which the left or right side appears higher from the back when the child bends over to touch their toes
The way clothing hangs on your child may also reveal signs of the condition. For example, a hem may look uneven, or one pant leg might appear longer.
Most children with scoliosis do not have any pain. However, in severe cases, the condition may cause breathing difficulties or pain in the back or shoulders. Your child may also feel tiredness or weakness in his or her back after sitting or standing for long periods.
If your child’s doctor detects scoliosis, the next step is to take X-rays to capture a clear image of the spine and measure to see if a curvature is present and how large it is. Your child’s doctor may also order other imaging tests to gather more information.
Treatment is really dependent on two main factors: the amount of remaining spine growth the child has and the size of the curve. More spine growth and larger curves are more likely to progress and get bigger. Curves are measured in degrees. A straight spine is 0 degrees, and any curve measuring above 10 degrees is considered scoliosis.
Treatment generally falls into these four categories:
- Observation - X-rays are taken every 4 to 8 months to monitor the curve. This is generally for curves less than 20 degrees.
- Bracing - Bracing is typically for curves between 20 and 45 degrees. If your child is still growing, scoliosis bracing may help prevent their curve from worsening. There are several types of scoliosis braces. At Scottish Rite for Children, all braces are custom made on-site in our Orthotics & Prosthetics lab by orthotists who work side-by-side with our physicians.
- Surgery - Surgery is generally used for curves above 45 to 50 degrees. The goal of surgery is to prevent the curve from worsening and to correct the curve a certain amount. The type of surgery most commonly used is a posterior spinal fusion with instrumentation. A newer technique, which is only indicated for some scoliosis cases, is vertebral body tethering (VBT.)
- Physical therapy - A scoliosis-specific exercise program can help your child’s symptoms and may be recommended along with bracing.
- Casting - Younger patients with scoliosis may be candidates for casting. This treatment includes a series of casts during the course of several months to slow or stop the curve from worsening.
Some children and teens feel embarrassed or self-conscious about having scoliosis or wearing a brace. Having mental health support can help them cope. Our peer support program is another resource we offer to patients and families to help them navigate scoliosis treatment.
In scoliosis patients with a curve of 50 degrees or more, spinal surgery is often the best treatment option. Surgery is also used for patients who did not achieve success with bracing. If surgery is needed, your surgeon will tailor the operation to the specific needs of your child.
- Spinal fusion surgery is the most common surgery performed to treat scoliosis. During this surgery, the curved vertebrae are fused together to create a single, solid bone. This stops the growth in the abnormal part of the spine and prevents the curve from worsening. Metal rods attached by screws are used to hold the spine in place until the bone heals.
- Vertebral body tethering (VBT) is a surgical treatment for idiopathic scoliosis in growing children. In this procedure, a surgeon attaches a flexible cord to the spine. The cord placement slows growth on one side of the curve while allowing growth on the other side, to potentially straighten the spine over time.
- Growing rods are used for patients diagnosed with early-onset scoliosis (EOS) – children under the age of 8. This is an innovative treatment that reduces the number of surgeries a child must undergo. In this procedure, a surgeon places a metal rod next to the spine. This rod can be lengthened as your child grows. There are two main types of growing rods: the traditional growing rod (TGR) and the MAGEC™(MAGnetic Expansion Control) rod.
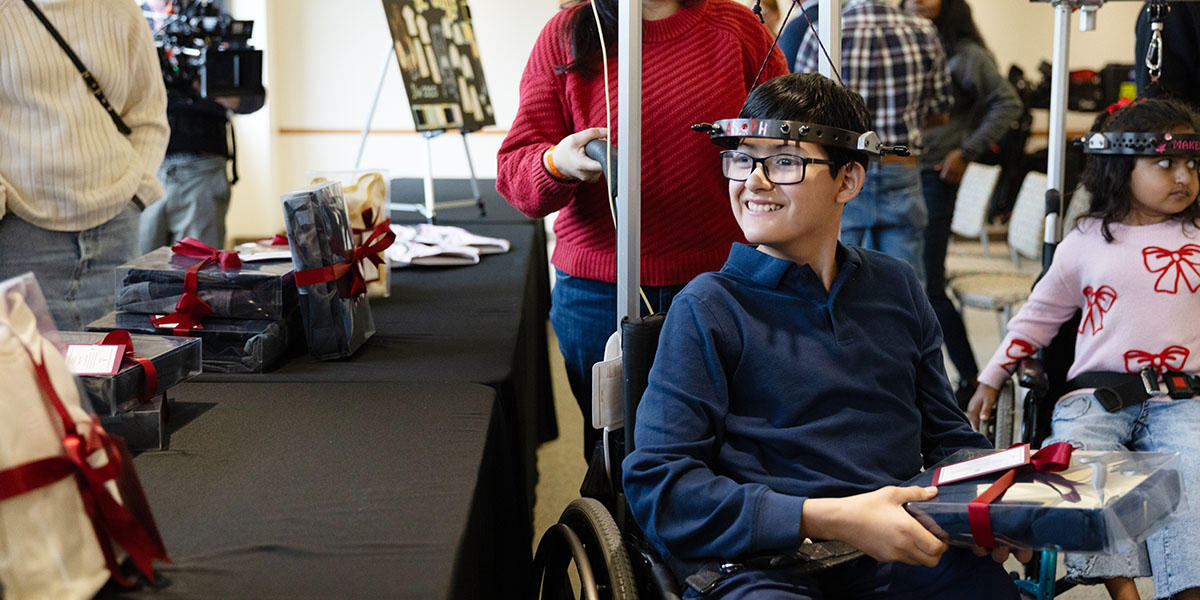
- Halo-Gravity Traction is the process of gently stretching and straightening a significantly curved spine, as seen in patients with scoliosis and kyphosis. This method of treatment is usually the first step in a treatment plan before other treatments, such as bracing, casting or spinal surgery. After the halo is placed, a traction device is attached using a pulley system that attaches to the child’s bed, wheelchair or walker. Over time, clinicians will add weight to the pulley to slowly stretch and straighten the child’s curved spine. During this process, clinicians will monitor your child’s movements and strength as well as take X-rays to track progress. Once your child’s curve has improved, the halo will be removed, and the next method of treatment will begin.
Scoliosis and spinal care experts at our Sarah M. and Charles E. Seay/Martha and Pat Beard Center for Excellence in Spine Research are working to:
- Detect symptoms earlier
- Determine the cause of idiopathic scoliosis
- Identify risk factors
- Improve treatment options
- Prevent progression of the condition
Our team is at the forefront of scoliosis research and technology. We have:
- Developed the Scottish Rite for Children Spinal System, which was the most widely used implant to treat spinal conditions.
- Identified three genes associated with idiopathic scoliosis, including the first detected associated gene in 2007.
- Improved innovative spinal surgical techniques, which have reduced blood transfusions during surgery for AIS patients, decreased the need for narcotic consumption post-surgery and minimized unnecessary blood draws in the hospital.
Our Center for Excellence in Spine Research is also home to the Pediatric Scoliosis Database and Genetic Scoliosis Database, informing and strengthening research to improve the care and lives of young people living with scoliosis. Both psychologists and child life specialists are available at Scottish Rite for Children to help patients cope with their diagnosis and treatment.
Mother-Daughter Scoliosis Journey
Ashley was treated for scoliosis by Dr. Dan Sucato in 2004. When her daughter was diagnosed with scoliosis 20 years later, she knew exactly where to bring her.
FAQs
What are the different types of scoliosis?
Is scoliosis genetic? Why do kids get scoliosis?
What are the signs and symptoms of scoliosis?
Is scoliosis painful?
When do I need to see a scoliosis specialist?
What do I need to do to become a patient?
Will I have to wear a back brace? Will it hurt?
What are the goals of scoliosis surgery?
Will I get a scar from surgery? How big will it be?
What activities can I do after surgery?
Our Experts

Daniel J. Sucato, M.D., M.S.
Jaysson T. Brooks, M.D.

Megan E. Johnson, M.D.

Amy L. McIntosh, M.D.

Jason R. Petrasic, M.D.
Brandon A. Ramo, M.D.
Karl E. Rathjen, M.D.

Shawne Barron, M.S.N., APRN, PCNS-BC
Cherlyn Caneda, CPNP, RNFA

Emily Chapman, CPNP-PC

Emily Holmes, CPNP-PC, A.C.

Jessica Landson, MPAS, P.A.-C.
Hong Putnam, P.A.-C
Latest news: Scoliosis & Spine
D CEO: Scottish Rite and TWU Team Up for Adaptive Fashion
At Texas Woman’s University, a fashion design class took learning beyond the classroom by focusing on how their skills could help the community. The course partnered with Scottish Rite for Children after…

How Danielle Unlocked Her Passion Through Scoliosis Treatment
Sixteen-year-old Danielle is an innovator at heart. During her scoliosis treatment, she discovered solace in the hum of motors at her school’s robotics club. “Robotics helped me power through my treatment,” Danielle…

D CEO: 2025 Excellence in Healthcare Award Winners Announced
D CEO revealed its 2025 Excellence in Healthcare Award winners. The program recognizes outstanding healthcare executives, practitioners, organizations and other innovative industry leaders in the Dallas region. Attracting more than 100 nominations, D…

CBS11: BMW Dallas Marathon Spotlights Children’s Resilience
As runners prepare for the BMW Dallas Marathon, organizers highlight that not all victories happen on the course. Proceeds benefit Scottish Rite for Children, which is spotlighting young patients whose resilience inspires…
Becker’s: Leading Pediatric Orthopedics at Scottish Rite with Dr. Daniel Sucato
Chief of Staff Daniel J. Sucato, M.D., M.S., speaks with Scott Becker on the Becker\'s Hospital Review Podcast about Scottish Rite for Children, ranked No. 1 in the nation for pediatric orthopedics…

CBS11: North Texas Teen Overcomes Spinal Surgery to Run in BMW Dallas Marathon
Seventeen-year-old Riley is preparing for the BMW Dallas Marathon, an achievement she once thought impossible. Diagnosed with scoliosis in seventh grade, Riley endured worsening pain until spinal surgery at Scottish Rite for…

Scottish Rite for Children Wins Award for Reducing Opioid Use Following Scoliosis Surgeries
Scottish Rite for Children has received one of Texas’ highest honors in health care quality — the Texas Hospital Association’s (THA) Bill Aston Award for Quality — for its innovative program that…

Inside DFW: How Art Helped Lorena Heal
Now in its fourteenth year, Summer Colors showcases original artwork from both established and emerging artists, including Lorena, a young patient at Scottish Rite whose journey through treatment inspired her to give…

CBS Texas: Livvy and Georgia go from patients to performers
During their time at Scottish Rite for Children, 12-year-old Livvy and 13-year-old Georgia found inspiration from the doctors, nurses and fellow patients who supported them through scoliosis. \"This place will always have…

CBS19: High School Graduate Dreams of Radiology Career After Her Care at Scottish Rite for Children
18-year-old Fernanda was diagnosed with scoliosis in sixth grade. \"It was difficult, but I just had to keep going through it,\" Fernanda says. Her experience at Scottish Rite for Children transformed from…