Sports Shoulder

Shoulder Conditions & Treatments in Young Athletes
Read more about the pediatric sports medicine services we provide.
SHOULDER CONDITIONS
SHOULDER
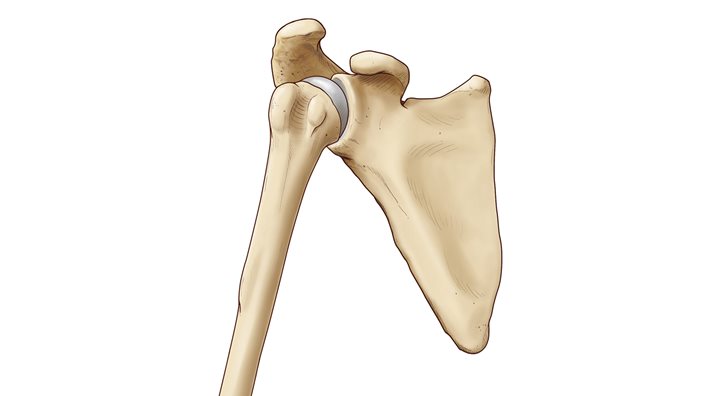
ANATOMY
CAUSE
PREVENTION
SYMPTOMS
DIAGNOSIS
TREATMENT
RETURN TO SPORTS
CAUSE
PREVENTION
It is unclear if this change in shoulder motion is necessary for successful pitching. Therefore, preventing symptoms related to this change is the goal. Recognizing signs and symptoms and responding promptly with proper rest are the most important steps.
SYMPTOMS
Generalized pain in the front of the shoulder may be a sign of changes in the shoulder, or it may be the sign of an injury.
DIAGNOSIS
A thorough history for an athlete includes a conversation about past medical history, the injury or onset of symptoms, as well sport exposure. Sport exposure includes what position, frequency of practices and games, length of seasons, and number of pitches, for baseball. Imaging will be ordered when the physical exam suggests other tissues may have been damaged.
TREATMENT
Treating the change in motion may not be necessary, unless the symptoms are directly related to the changes in motion. Treatment is typically recommended so that the athlete can learn exercises to reduce his risk of injury because of the excessive rotation in one direction. This would include shoulder blade stabilizing exercises, among other exercises.
RETURN TO SPORTS
ANATOMY
CAUSE
PREVENTION
Strengthening exercises for the shoulder’s rotator cuff muscles and muscles around the shoulder blade can improve stability. These exercises can also improve the body’s ability to respond to changes in movement. This is a combination of proprioception and neuromuscular control.
SYMPTOMS
Severe pain with a traumatic dislocation often improves quickly when the shoulder is returned to its normal position. With repetitive dislocations, there may be no pain because the tissues have changed over time to allow this movement to occur easily.
DIAGNOSIS
A thorough conversation about episodes of instability and dislocation will help a provider confirm the diagnosis. X-ray or other imaging of the shoulder may be ordered to help to rule out a fracture and to evaluate the joint surfaces and soft tissue for changes.
TREATMENT
With early recognition, physical therapy can help to improve pain, motion and stability. Most athletes return to play after an initial event. In cases of repetitive events, surgical reconstruction may be required. Physical therapy after a reconstruction will help to regain shoulder mobility and strength.
RETURN TO SPORTS
In non-operative treatment plans, sports participation may only be limited for a short period of time to allow focused rehabilitation. After a surgical procedure, restrictions from sports and other activities will vary from 4-6 months, and returning to sports will be most safe after completing a rehabilitation program designed specifically for the athlete.
ANATOMY
CAUSE
PREVENTION
Stabilization exercises for the shoulder and shoulder blade can improve the strength of the muscles. More importantly, the stabilization exercises can put the shoulder in its best position, both for performance and for injury prevention.
SYMPTOMS
Pain with activity, especially throwing and overhead activity. Pain and instability are common with labral tears. Range of motion is usually normal.
DIAGNOSIS
A thorough conversation about symptoms, activities and any injuries can help a provider make a preliminary diagnosis. Radiographic X-rays and an MRI may be ordered to assess the bone and soft tissue, including the labrum. There are names for damage to different areas of the labrum. SLAP or Bankhart lesions are the most common tears in adolescent athletes.
TREATMENT
Not all labral tears will require surgery. The athlete’s symptoms, like pain and instability, and ability to perform daily activities, will help to determine if surgical treatment is required.
RETURN TO SPORTS
In non-operative treatment plans, sports participation may only be limited for a short period of time to allow focused rehabilitation. After a surgical procedure, restrictions from sports and other activities will vary from four to six months, and returning to sports will be most safe after completing a rehabilitation program designed specifically for the athlete.
ANATOMY
CAUSE
PREVENTION
Proper equipment for the position played and proper tackling form for the tackler and the player being tackled can reduce the risk of an AC joint separation.
SYMPTOMS
Typically, there is severe pain and limited ability to move the shoulder at the time of injury. Swelling and bruising follow soon after.
DIAGNOSIS
The joint may appear abnormal in a visual exam. With a physical exam, there is tenderness at the AC joint. An x-ray is typically ordered to rule out a clavicle or collarbone fracture. An AC joint separation is categorized based on the severity of the injury.
TREATMENT
In the early phase, rest and activity restrictions are recommended. Immobilization in a sling helps to rest the shoulder during healing. Most cases will heal on their own with these treatments and surgery is rarely needed.
RETURN TO SPORTS
Follow-up physical exams are important to assess the tightness of the healing ligament and the mobility of the shoulder. Returning to sports before healing puts the shoulder at risk of a more severe injury.
ANATOMY
CAUSE
PREVENTION
Proper equipment for the position played and proper tackling form for the tackler and the player being tackled and reduce the risk of a burner.
SYMPTOMS
Neurological symptoms include numbness, tingling and pain in the arm, only on one side. These typically last less than 15 minutes, but in some cases, may last days or weeks. Because the injuries can occur together, the athlete should be evaluated for signs and symptoms of a sports concussion.
DIAGNOSIS
The mechanism of the fall, combined with the description of one-sided neurological symptoms, is typically sufficient for a diagnosis. Imaging may be recommended to rule out other problems in the neck and for patients with persistent symptoms or a history of multiple stingers.
TREATMENT
In the early phase, rest, a sling for comfort and NSAIDS may be used. Typically, healthy athletes will recover quickly and will not need treatment. Surgical treatment for this is extremely rare. Rehabilitation may be recommended for neck and shoulder strengthening.
RETURN TO SPORTS
Without signs and symptoms of another injury, athletes can typically return to sports quickly when they are symptom free.
ANATOMY
CAUSE
PREVENTION
In some sports, like football, pads and gear may protect the collarbone. In other sports, proper balance of strength and flexibility of the neck and shoulder muscles may aide in preventing collarbone injuries. These injuries are often unpredictable, and likely unpreventable.
SYMPTOMS
DIAGNOSIS
X-rays are most useful in confirming the diagnosis and to guide treatment planning.
TREATMENT
Non-operative approaches include using a sling to immobilize the arm for comfort, and monitoring the natural healing process of the bone. This has been shown to be effective in most cases. Surgical intervention is considered where natural healing is not likely to promote normal function of the shoulder.
RETURN TO SPORTS
After a period of 6-8 weeks, with pain resolved and x-ray evidence of good bone healing, an athlete is often returned to sports with instructions to progress as tolerated. For some collision sports like hockey and football, a longer healing time may be recommended.

SHOULDER INJURY PREVENTION
- Perform proper warm-up and stretching.
- Learn and maintain proper form.
- Stop activity when tired and form becomes worse.
- Avoid year-round play.
- Avoid playing on multiple teams during a single season.
- Do not focus on a single sport until at least 14 years old.
- Cross train and perform exercises to help with lower body, shoulder and scapular stabilization.



.jpg?width=1200&height=619&ext=.jpg)